9 March 2026
Nicholas Howlett, James Cameron, and Richard Wood delve into their research, published in the EMJ, on the link between longer stays in A&E and mortality rates*
Delaying sick medical patients in the ED for many hours is, on the face of it, clearly a bad idea. It leads to crowding and corridor care, but is it really more than a logistical inconvenience? And even if it is shown to have significant, real-world harms, is there actually anything we can do about it without spending billions of pounds on more and more hospital beds?
What we are talking about:
The average medical admission from the ED in our study took 3.5 hours to Decision To Admit (DTA) and spent 9.7 hours in the ED altogether.

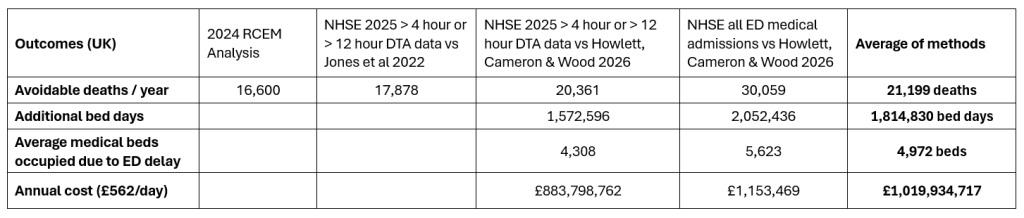
1. How much harm is done by delaying medical patients in the ED while they wait for an inpatient bed?
Let’s look at four different ways to work out the estimates of harm (additional deaths and increased length of stay) on inpatient wards.
2. It’s not that there are boarding delays in the ED because there aren’t enough beds in the hospital, It’s that there aren’t enough beds in the hospital because there are boarding delays in the ED.
Our paper showed that for every 4 hours spent boarding in the ED waiting for a medical bed, the inpatient length of stay increases by 8.6 hours. Our average patient boarded for 6.2 hours and so their admission extended by 13.3 hours as a result.
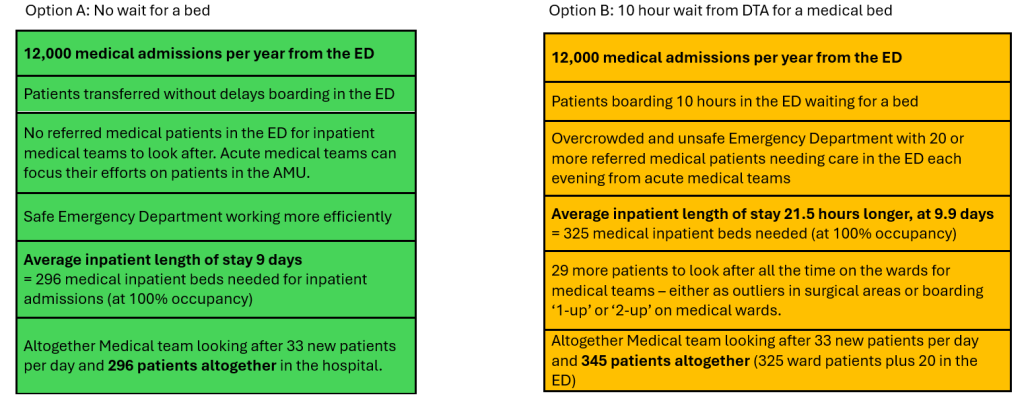
3. Example Hospital = 12,000 admissions from the ED to Medical Wards each year, equating to 33 per day (excludes GP referrals).
Our paper showed 56% of medical patients waited more than 4 hours from DTA for a bed, and that this delayed group had a number needed to harm (NNH – mortality) of 69. In other words, for every 69 patients boarding more than 4 hours, 1 additional death will occur.

It is surprising to see how consistent hospitals are in the number of patients waiting for a medical bed, requiring the time spent in escalation measures at Opel 3, 4 and into critical incident to prevent it reaching into hundreds of patients boarding in each ED. UK acute hospitals are consistently run with a backlog of referred medical patients waiting in the ED month after month, and year after year. It is how NHS hospitals work.
4. Doctor’s Mess Sink Analogy
Every year thousands of cups, bowls, spoons and forks are used in the doctors mess. With busy people on call sometimes rushing off to emergencies mid meal the washing up can accumulate. If you want a clean cup or bowl you have to rummage around in the dirty dishes and find one and clean it before you can have a cup of tea. It’s awkward and takes longer than if the sink was clear and all the crockery was clean to use. You might even break a glass and cut your finger. It’s not deliberately done. People intend to always keep up and never fall behind but tend to fall behind when times are busy and there’s lots of different people involved.

This falling behind is what happens in hospital wards every day, and patients become backed up in the emergency department ‘sink’.
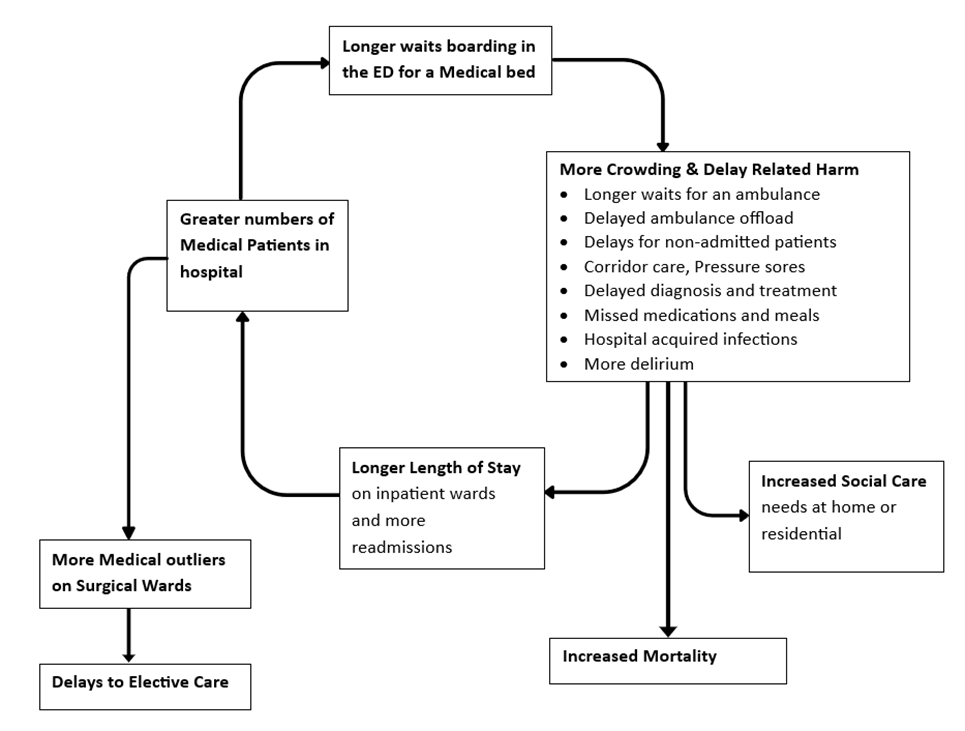
5. The Vicious Cycle of Delay Related Harm
It all starts with boarding delay in the ED awaiting a medical bed, that harm worsens outcomes, length of stay and the ability of the hospital to function effectively across all its domains. We really are shooting ourselves in the foot.
6. What if Acute NHS Hospitals did things differently and just stuck to it?
In our paper we found that for each hour a patient spends boarding in the ED waiting for a medical bed, their inpatient length of stay (after leaving the ED) was 2.15 hours longer.
7. Frequently Asked Questions
- a) But we don’t have any empty beds today. Where do we get the beds for all these medical patients stuck in the ED right now?
Hospitals need to catch up with the backlog in the ED just once and stick to it. You can catch up by one patient a day. For the example hospital admitting 12,000 a year from the ED to medical wards, they already admit 33 patients a day. With a longstanding backlog of 20 medical patients boarding in the ED, admitting one extra patients per day for 3 weeks means the hospital has caught up and inpatient length of stay will drop, improving things within weeks and for the long term. An extra 20 patients over 3 weeks is within the normal variation of attendances and will be well tolerated. - b) Is this just spreading the risk? If we move all the excess patients from the ED won’t we just have excess patients on corridors in medical wards instead?
Boarding delays in the ED awaiting a medical bed mean patients spend significantly longer on the wards. Stopping ED boarding will reduce the amount of boarding that happens on the wards. This is not a ‘zero-sum’ situation in which harm and crowding are inevitable – we can manage the patients we currently look after in a much more efficient and compassionate way. Permanent backlogs are a sign of a lack of organisation and operational discipline. - c) Isn’t it safer to keep all the excess patients in one place? (the Emergency Department)
– Stopping boarding in the ED reduces boarding on the wards and outliers.
– Although it is much safer for 20 wards to have one extra patient than one ward to have 20 extra patients, whether that is the ED or any other ward, the best plan is to stop ED boarding and thereby reduce crowding on the inpatient wards. - d) Don’t we need to fix social care first before we can improve things in the ED?
Our study was standardised for the number of patients with no criteria to reside. Many acute hospitals have significant numbers of inpatient beds occupied by patients who should have been discharged to social care, either at home or residential. Regardless of this, boarding patients in the ED causes prolonged inpatient length of stay and worsens any underlying bed shortage. - e) If it makes things better, why aren’t we doing this everywhere already?
It is difficult for a hospital to maintain the discipline of moving patients from the ED to keep up with daily demand. There is a natural desire to keep individuals in hospital a bit longer for scans or further assessments and so backlogs tend to build up. Hospitals have inadvertently developed systems and a culture that rely on the ‘moral authority’ of things being very crowded and unsafe in the ED to escalate to Opel 3,4 and critical incident escalation levels to keep up with the daily demand. - f) Will the ED admit more patients if it’s made easier to admit them?
When it is overcrowded in the ED, staff have less time and headspace to manage and discharge patients. It seems easier to just admit them. When it is more overcrowded there are more referrals. This is yet another example of the ‘vicious cycle of delay-related harm’ in action. - g) Can boarding medical patients in the ED really be that bad if everyone is doing it?
This is an example of the ‘bandwagon fallacy’ – just because everyone is doing it doesn’t mean it’s safe. Just like smoking cigarettes or using asbestos in the 1950s, there is no safety in numbers here.
Further notes on calculations to calculate national numbers
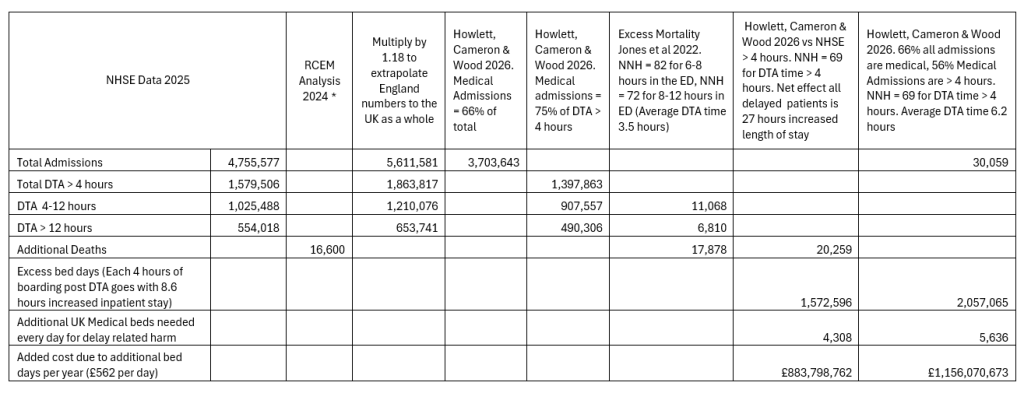
Links / References
Medical patient boarding in the emergency department as a source of crowding and delay-related harm, impacting patient outcomes and the efficiency of urgent and emergency care | Emergency Medicine Journal Howlett, Cameron & Wood EMJ 2026
Association between delays to patient admission from the emergency department and all-cause 30-day mortality Jones et al EMJ 2022
Monthly-AE-Time-Series-January-2026-C86cfU.xls NHS England Data
James Cameron, Richard Wood, Nick Howlett February 2026
*The research explored in this piece are the authors own. To see RCEM’s response to this study, click here.