13.05.26
By Dr Rhodri Morgan‑Smith, Emergency Medicine clinician
Content note: this blog describes acute trauma, pain, and emergency treatment. Some clinical abbreviations and technical terms are used in this blog. A short glossary explaining these appears at the end for readers who would find it helpful.
As an emergency medicine clinician, I’ve spent years caring for trauma patients. I never expected to become one myself. What follows is the story of the day my role reversed — and what I learned from being on the trolley rather than beside it.

The Injury
It’s an overcast December Saturday, and the second half of an amateur rugby union match is kicking off. The away side have just brought on their one substitute. The home team kick straight to the new sub. He is hit hard in a tackle and falls to the ground, the tackler landing on his right leg.
He’s screaming. His right leg doesn’t look right. The tackler mutters something about “just walk it off”, while people from the home team ask, “Haven’t you lot got a doctor playing for you?”
The away team point to the injured player on the floor.
“Yeah — he’s the one on the ground.”
Me.
I’m in a world of pain and utterly uncomprehending of what has happened — an immediate explosion of pain in my right hip and a sudden fizz as a large area of my lower leg becomes numb.
From this point onwards, my experience becomes an education: experiencing firsthand what it is to be on the other side of the trolley. I’m lucid throughout, though time feels elastic — seconds last forever, while hours disappear.
Lying on the pitch, I’m still slightly in doctor mode and tentatively try to move my hip. My leg is held internally rotated and flexed at both hip and knee. This is a mistake. Any movement takes me to 10/10 pain. My brain, slightly dissociating, thinks: “So that’s what 10/10 pain truly is,” and stores it away as a learning need met rather than psychological trauma.
Supporters gather around me, keeping me warm and calling 999. Because of the ongoing crisis in ambulance services, the estimated wait is two to three hours. Someone retrieves my belongings. I ring my wife — who is on shift at another hospital — to tell her that I think I’ve broken my hip.
Waiting for Help
I’m stretchered into the clubhouse. My world has shrunk to what I can see lying on my side with my hip and knee bent; any movement brings agony. I feel very vulnerable, even with all my knowledge of the process which I’ve suddenly become a part of.
The crew arrive much quicker than expected — about half an hour. They assess me, cannulate me, and get me onto Entonox and IV morphine. They tell me it looks more like a dislocation than a fracture.
I don’t wear my ‘doctor’ identity outside of work, and I’m happy to be somewhat passive in this trauma situation. In fact, I’m determined to push this part of my life aside and just be a patient. I’m not going to make people uneasy by telling all and sundry that I’m an EM consultant. I’m not making demands or comments about cannulation skills or methods of getting me onto the stretcher.
Like all of us, I’ve been the clinician whose cognitive space has been affected by someone waving their lanyard the moment we enter the cubicle. That’s not how I roll.

In the Emergency Department
Then it’s onward to the local ED. I’m swiftly handed over and transferred onto a hospital trolley. More IV morphine. I’m seen almost immediately by the ED consultant and moved to Resus.
I am cared for by an exceptional ED nurse. At this point I am in pain, fully dependent, and very, very vulnerable — and this nurse becomes my anchor. Doctors come and go, in and out of the cubicle. The nurse — my nurse — is a constant in my tunnel‑visioned existence in that moment.
They are there. I feel safe.
I have a rather clichéd but strong and valid memory of them smiling sympathetically at me. I had sworn a series of F‑words after a paroxysm of pain and was embarrassed and distressed by this. They made sure I knew it was okay — that this was obvious severe pain, and that I was simply communicating it.
An X‑ray is booked and more analgesia given. By this point, I’ve had 25 mg IV morphine and 80 micrograms IV fentanyl.
Imaging
I’m wheeled through to X‑ray. The radiographer wants me flat on my back. I’m like a cornered animal, clutching the trolley bars and begging them not to. I scream in pain when they try — loud enough that my wife later tells me she could hear it from Resus.
My nurse advocates for me, and a less‑than‑ideal view is agreed as the best option for me, the patient.
In retrospect, I really appreciate the pragmatism. It’s something we as emergency clinicians do all the time — we often don’t need perfect images or results. We need enough information, combined with clinical gestalt, to act in a timely, patient‑centred way.
In this case, perfect was the enemy of good.
Back in my cubicle, I hear a loud voice say clearly,
“Is that the hip?”
My wife was standing outside the cubicle and was being addressed by the questioner. She later described how abrupt it felt. Dot corrected this person, who was in fact pointing at a different patient — dumbfounded at the way a stranger had reduced me to a joint, to pathology alone.
The Diagnosis
The voice belongs to a clinician not involved in my care, who barges into my cubicle, followed by Dot. They look at my wife and ask,
“Is he medical?”
Without waiting for an answer, they announce:
“This is the worst X‑ray I’ve ever seen. You’ve got a life‑changing injury.”
They then walk off, calling people over to the computer‑on‑wheels immediately outside my cubicle to look at my X‑ray.
I ask my nurse,
“Who the **** was that?”
This moment absolutely astonished me. The glee this person took in a rare pathology completely over‑rode their basic duty of care toward me. We only knew who they were from the ID badge dangling on their lanyard.
The contrast between this and the exceptional care from the rest of the team — particularly the nurse looking after me — was stark.
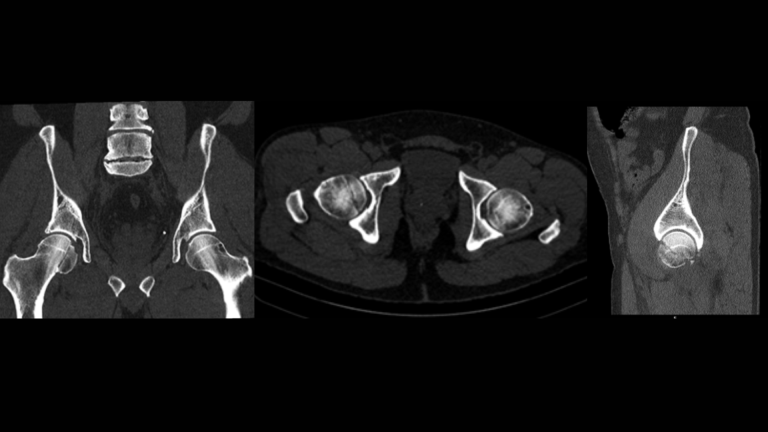
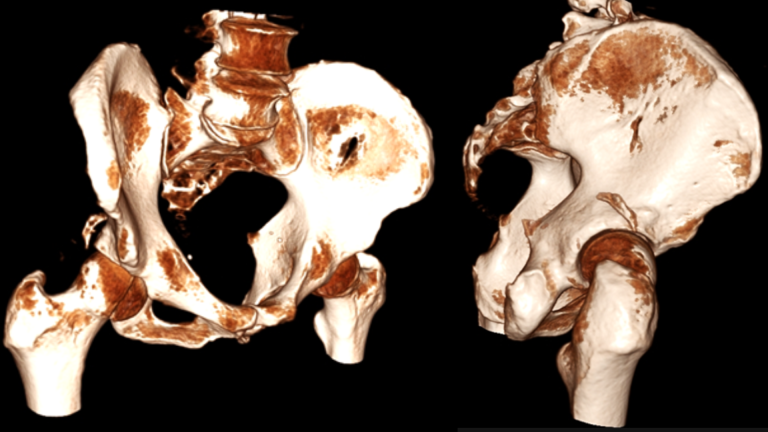
Soon after, my own doctor reviews me, followed by the orthopaedic team. They explain the injury: my femoral head has been sheared in two — part remaining in the joint, the rest of the femur dislocated posteriorly — with associated pelvic fractures. I have foot drop and numbness, raising concern for common peroneal nerve injury.
Given the rarity of the injury, it is explained that best practice is evolving and should be patient‑centred under the direction of specialist hip surgeons. An urgent reduction is planned — it is time‑critical to reduce nerve injury risk and promote fracture healing.
In a serendipitous example of NHS diversity improving patient care, the orthopaedic registrar caring for me has seen several similar injuries while working in India — all from high‑energy trauma, never from sport.
The Pipkin classification describes femoral head fractures, usually caused by high‑energy trauma such as falls from height or road traffic collisions. Historically linked to dashboard injuries, they can still occur when a passenger’s feet are braced against an airbag, which inflates at 100–200 mph.
These injuries are rare in sport, as they require force along a fixed axis; only a small number of rugby cases have been reported. A well‑known example is Tua Tagovailoa, who sustained a Pipkin IV fracture while playing college football.
Pipkin fractures are classified Type I–IV by fracture position and associated femoral neck or acetabular injury.
They carry a high risk of avascular necrosis, heterotopic ossification, degenerative joint disease, and neurovascular injury. Urgent reduction is essential — delays beyond six hours significantly increase AVN risk. Management should be specialist‑led and patient‑centred.

From Theatre to the Ward — and Beyond
Everything moves quickly. I’m seen by anaesthetics, wheeled to theatre, and anaesthetised.
I wake up in recovery with my leg in traction to prevent movement. The relief from the reduction is immediate and profound. Then it’s off to the ward — and on to the next stage.
After four days in traction on the neck of femur ward and a post‑reduction CT, I’m repatriated to a regional pelvic centre closer to home.
After discussion with the specialists, and weighing non‑operative management against ORIF, we opt for conservative treatment. I make it home four days after the injury — on Christmas Eve — initially in a cricket splint to prevent hip flexion, and later fitted with a hip brace.
Mobility is initially extremely limited, but the brace allows a little more freedom within the confines of my home.
By March I’m making a steady recovery. A CT scan has shown that the femoral head has somehow re‑united with minimal avascular necrosis, and the hip is stable. I’m mobile without aids and can walk short distances, though I fatigue and develop pain quickly. There is still a great deal of rehabilitation work ahead.
The foot drop improved slowly and then plateaued. I’m prepared for the possibility of a lifelong limp, and for never being able to cycle, jog or run again. Neuropathic pain ruled my existence for weeks — allodynia, absent sensation, sleepless nights — and it is only now starting to come under control.
My world became very small. Limited mobility and dependence on others for transport were difficult to reconcile with who I was before. Non‑sport hobbies, the support of friends and family, and the ability for people to reach me through social media mattered enormously. I will be forever grateful to those who were there for me during those first three months.
For now, the pelvic team are taking a watch‑and‑wait approach over the next two years, with the option of total hip replacement should the joint fail.
I am still likely several months away from resuming my career. I’ve hung up my rugby boots — but I’m not ready to hang up my stethoscope.
Five lessons from the other side
- Patients hear more than we think: Curtains are not soundproof, and clinical discussions need careful thought about timing, place, and audience.
- Words matter: Casual remarks can cause lasting emotional harm, undermine dignity, and breach confidentiality — even when no harm is intended.
- Patients are people, not pathology: They are not their imaging or blood results, and reducing them to these strips away humanity.
- Advocacy is care: Nurses demonstrate this every day through presence, protection, and human connection — and it makes a profound difference.
- Vulnerability can arrive suddenly: A clinician‑patient is a patient first. Care, compassion, and dignity are not optional extras — they are treatment, and this can happen to any of us.
About the Author
Dr Rhodri Morgan‑Smith is an Emergency Medicine clinician with 15 years’ experience working in major trauma centres and trauma units. He has most recently worked as a locum consultant in the West Midlands and Norfolk, with particular interests in toxicology and advanced clinical practitioner education. He lives in Cheshire with his wife, Dot, and their two greyhounds.
Share Your Story
This blog is part of RCEM’s Share Your Story campaign, an initiative that invites the EM community to share their written or video experiences to help build inclusion, understanding, and equality across our specialty. We welcome contributions for medical awareness and diversity days throughout the year, chosen in collaboration with our EDI Committee and NHS Employers.
This short glossary explains clinical terms and abbreviations used in the blog. It is included for clarity and accessibility and is not intended as a comprehensive medical reference.
ED (Emergency Department)
The hospital department providing urgent and emergency care.
Resus (Resuscitation area)
A high‑acuity area of the Emergency Department used for critically unwell or seriously injured patients.
IV (Intravenous)
Medication or fluids given directly into a vein.
CT (Computed Tomography)
A type of imaging scan that uses X‑rays to create detailed cross‑sectional pictures of the body.
RTC (Road traffic collision)
An incident involving vehicles on the road, sometimes called a road traffic accident.
#NOF (Neck of femur fracture)
An orthopaedic term for a fracture of the upper femur, most commonly seen in older adults.
Pipkin fracture / Pipkin IV
A classification system describing fractures of the femoral head (the ball of the hip joint). Type IV indicates an associated acetabular (hip socket) fracture.
Femoral head / acetabulum / fovea
Anatomical terms relating to the hip joint: Acetabulum – the hip socket, Femoral head – the ball at the top of the thigh bone, Fovea – a small indentation on the femoral head where a ligament attaches.
Posterior dislocation
A displacement of the femoral head backwards out of the hip socket, usually caused by high‑energy trauma.
Intracapsular injury
An injury occurring within the joint capsule, which can affect blood supply and healing.
Axial loading
Force transmitted along the length of a bone or joint, often associated with high‑energy impacts.
Reduction
The process of moving a dislocated joint back into its normal anatomical position.
Traction
A method of applying controlled pulling force to a limb to maintain alignment and reduce pain.
ORIF (Open Reduction and Internal Fixation)
A surgical procedure in which broken bones are repositioned and secured with plates, screws, or other hardware.
THR (Total Hip Replacement)
Surgical replacement of the hip joint with a prosthetic joint.
AVN (Avascular necrosis)
Bone death caused by disruption of blood supply, a recognised complication of hip dislocation and femoral head fractures.
Common peroneal nerve
A nerve supplying movement and sensation to parts of the lower leg and foot.
Foot drop
Weakness or inability to lift the front of the foot, often due to nerve injury.
Neuropathic pain
Pain resulting from nerve damage rather than tissue injury.
Allodynia
A type of neuropathic pain where normally non‑painful stimuli (such as light touch) are perceived as painful.
ADLs (Activities of Daily Living)
Everyday self‑care tasks such as washing, dressing, and moving around the home.
Clinical gestalt
A clinician’s overall impression based on experience, pattern recognition, and assessment rather than a single test result.
Repatriated (between hospitals)
Transferred back to a hospital closer to home or to a specialist centre for ongoing care.